A woman in her early 30s with a past medical history of Hashimoto’s thyroiditis and one prior miscarriage at <8 weeks presented with chest pain about 6 weeks postpartum from the birth of her third child. In the ED, she continued to report intermittent sharp chest discomfort and found to have a diastolic decrescendo murmur at the left upper sternal border and labs demonstrating a troponin-I of 0.07 ng/dL. Join the UMD Cardionerds for the incredible course and story of this young patient as we go through the differentia and approach to postpartum chest pain and ultimately arrive in a very rare diagnosis! For a detailed course, enjoy the JACC case report.
The CardioNerds 5! – 5 major takeaways from the #CNCR case
1. How Do We Evaluate Chest Pain in Younger Patients
Start with the same things as everyone else! Think broadly about the big three concerning etiologies of chest pain: Cardiac, Gastric, and Pulmonary (The excellent Clinical Problems Solvers 4+2+2 construct here is always a great resource. Find them at: https://clinicalproblemsolving.com/dx-schema-chest-pain/).
Of course it is important to think about non-life threatening etiologies as well – esophageal spasm, gastric ulcer, rib fracture, skin lesion, among many others – given that high-risk chest pain is less likely in younger adults.
While less common, acute coronary syndrome is not uncommon in young patients, as 23% of patients with MI present at age <55 years.
2. What About Chest Pain in Women?
As has been discussed on the Cardionerds podcast (Listen to episodes with Dr. Nanette Wenger, Dr Martha Gulati, and Dr. Leslie Cho), women generally present with acute coronary syndrome at a later age, with a higher burden of risk factors than men, and with greater symptom burden but are less likely to be treated with guideline-directed medical therapies, undergo cardiac catheterization and receive timely reperfusion. In one study of young patients with acute MI, women – 19% of cases overall – were less likely to undergo revascularization or receive guideline-directed therapy
The construct of classifying chest pain as “typical” and “atypical” likely leads to misdiagnosis or delayed diagnosis of acute myocardial infarction in women. Rather, it is important to recognize that while symptoms may not be “typical” for angina, coronary disease can manifest in many different ways.
While many women will presents with chest pain suggestive of angina, women are more likely than men to present with dyspnea, indigestion, weakness, nausea/vomiting and/or fatigue. Note, shoulder pain and arm pain are twice as predictive of an acute myocardial infarction diagnosis in women compared with men.
Furthermore, while obstructive epicardial disease remains the primary cause of acute MI in young women, it is also important to keep other causes of chest pain such as MINOCA, SCAD (see the UCLA episode), peripartum cardiomyopathy (see the Penn and MCW episodes), or coronary vasculitis on the differential. While these etiologies are rare, they are disproportionately represented in young women.
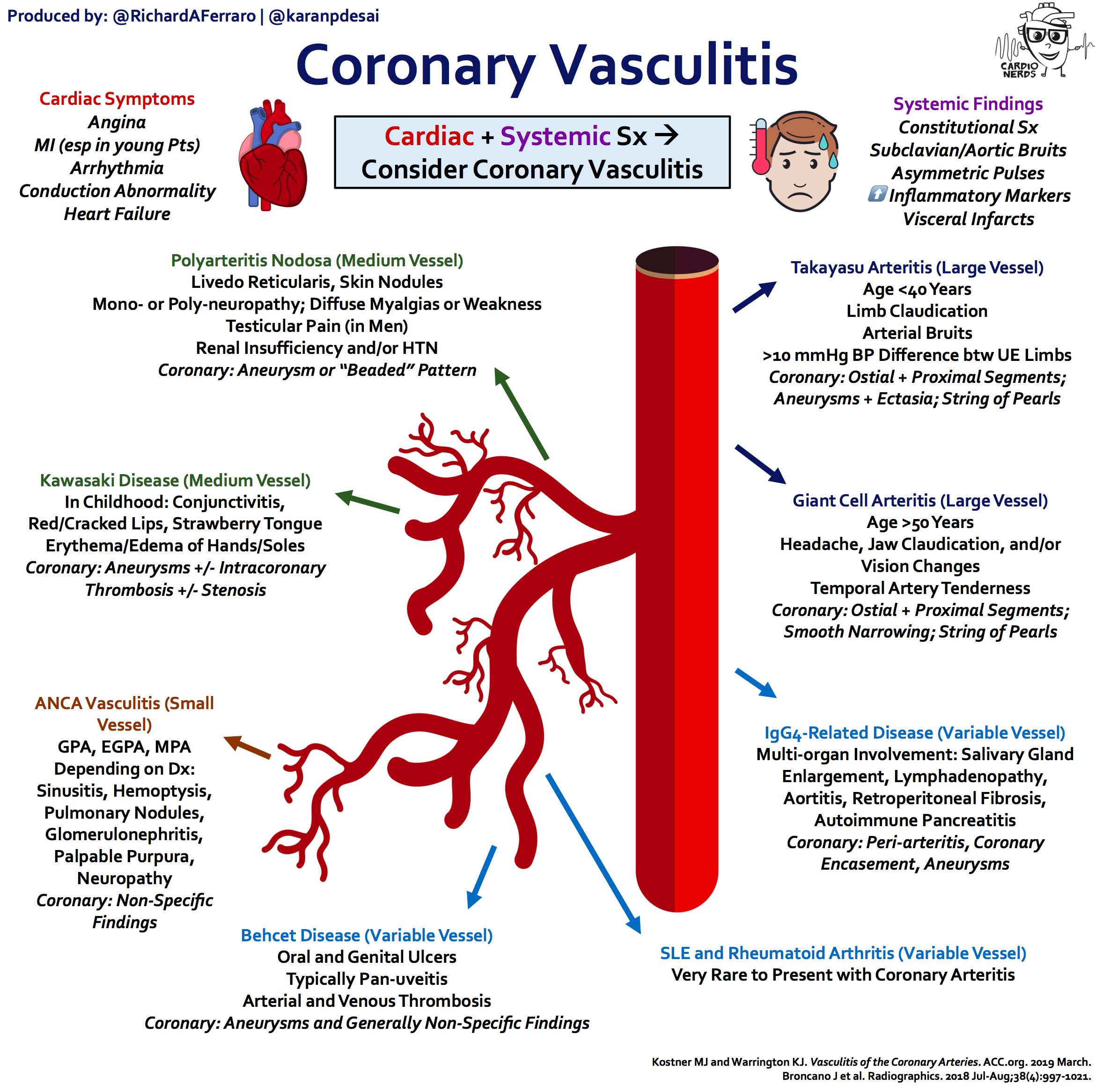
3. How do we think about categorizing vasculitis?
Vasculitis is a broad term encompassing many forms of vessel wall (including arteries, veins or capillaries) inflammation. This can be secondary to autoimmunity, infection, drug reaction, and malignancy to name a few underlying causes.
Generally vasculitis is divided by large vessel (e.g., Takayasu, Giant Cell), medium vessel (e.g., Polyarteritis Nodosa), and small vessel etiologies (e.g., Granulomatosis with Polyangitis, Eosinophilic Granulomatosis with Polyangiitis, Microscopic Polyangitis, Immune-mediated Vasculitis, amongst others). This characterization follows the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitis.
Other important categories includes variable vessel vasculitis (e.g., Behcet’s Disease, Cogan’s Syndrome) and vasculitis associated with systemic disease (e.g., Lupus vasculitis, Rheumatoid vasculitis, Sarcoid vasculitis).
4. What Does Vasculitis Look Like in the Heart?
While inflammation can occur throughout the heart – e.g., pericarditis or myocarditis – vasculitis in the heart refers specifically to inflammation of the coronary arteries. This is a relatively rare process, with <10% of vasculitis patients exhibiting cardiac involvement.
Patients with coronary vasculitis rarely present with isolated coronary involvement and typically have systemic manifestations, such as constitutional symptoms in addition to cardiac symptoms (e.g., angina, heart failure, arrhythmia). Examination may reveal asymmetric pulses or BP readings between limbs and arterial bruits, with imaging revealing multi-organ infarcts without a clear embolic origin. Amongst the vasculitides, Takayasu Arteritis (TA) is one of the more frequent etiologies of coronary arteritis.
In Takayasu Arteritis (TA), the affected arteries are typically the aorta and its major branches. In contrast to giant cell arteritis (GCA), TA is quite rare and tends to have onset <40 years age; however, for both diagnoses coronary involvement is rare. TA patients will typically have constitutional symptoms and may have diminished/absent arterial pulses often accompanied by bruits. Weakness of the arterial walls may lead to aneurysms and specifically aortic root aneurysm may result in aortic valve insufficiency. When involving the coronaries, there are three main type of TA lesions: stenosis or occlusion of the ostia/proximal segments (Type 1); diffuse or focal coronary vasculitis involving all the epicardial branches or focal areas (Type 2); coronary aneurysms (Type 3).
5. What Are the Complications of Coronary Vasculitis?
The consequences of coronary vasculitis are variable and much of the data we have comes from case reports. As in the case presented, severe coronary ischemia and its complications, including arrhythmia and cardiac arrest, are a major concern. However, cardiac arrest is rarely the first presentation of coronary vasculitis, especially if it is detected early. The manifestations of coronary vasculitis are also going to be dependent on the specific etiology of the arteritis.
Amongst the medium vessel vasculitis and specifically polyarteritis nodosa, 15-20% of patients will have cardiac involvement, with major complications including heart failure, myocardial infarction, or arrhythmia.
Amongst the small vessel vasculitis, eosinophilic granulomatosis with polyangiitis is the most common culprit for cardiac involvement, primarily secondary to eosinophilic toxicity. Cardiac involvement is a major cause of mortality and poor prognostic sign in EGPA.
The CardioNerds Cardiology Case Reports series shines light on the hidden curriculum of medical storytelling. We learn together while discussing fascinating cases in this fun, engaging, and educational format. Each episode ends with an “Expert CardioNerd Perspectives & Review” (E-CPR) for a nuanced teaching from a content expert. We truly believe that hearing about a patient is the singular theme that unifies everyone at every level, from the student to the professor emeritus.
We are teaming up with the ACC FIT Section to use the #CNCR episodes to showcase CV education across the country in the era of virtual recruitment. As part of the recruitment series, each episode features fellows from a given program discussing and teaching about an interesting case as well as sharing what makes their hearts flutter about their fellowship training. The case discussion is followed by both an E-CPR segment and a message from the program director.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}